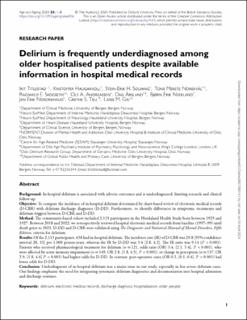
Delirium is frequently underdiagnosed among older hospitalised patients despite available information in hospital medical records
| dc.contributor.author | Haugarvoll, Kristoffer | |
| dc.contributor.author | Solvang, Stein-Erik Hafstad | |
| dc.contributor.author | Norekvål, Tone Merete | |
| dc.contributor.author | Skogseth, Ragnhild Eide | |
| dc.contributor.author | andreassen, Ole A | |
| dc.contributor.author | Årsland, Dag | |
| dc.contributor.author | Neerland, Bjørn Erik | |
| dc.contributor.author | Nordrehaug, Jan Erik | |
| dc.contributor.author | Tell, Grethe S | |
| dc.contributor.author | Giil, Lasse Melvær | |
| dc.date.accessioned | 2024-04-12T06:00:33Z | |
| dc.date.available | 2024-04-12T06:00:33Z | |
| dc.date.created | 2024-02-14T09:52:01Z | |
| dc.date.issued | 2024 | |
| dc.identifier.issn | 0002-0729 | |
| dc.identifier.uri | https://hdl.handle.net/11250/3126182 | |
| dc.description.abstract | Background: In-hospital delirium is associated with adverse outcomes and is underdiagnosed, limiting research and clinical follow-up. Objective: To compare the incidence of in-hospital delirium determined by chart-based review of electronic medical records (D-CBR) with delirium discharge diagnoses (D-DD). Furthermore, to identify differences in symptoms, treatments and delirium triggers between D-CBR and D-DD. Method: The community-based cohort included 2,115 participants in the Hordaland Health Study born between 1925 and 1927. Between 2018 and 2022, we retrospectively reviewed hospital electronic medical records from baseline (1997–99) until death prior to 2023. D-DD and D-CBR were validated using The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, criteria for delirium. Results: Of the 2,115 participants, 638 had in-hospital delirium. The incidence rate (IR) of D-CBR was 29.8 [95% confidence interval 28, 32] per 1,000 person-years, whereas the IR by D-DD was 3.4 [2.8, 4.2]. The IR ratio was 9.14 (P < 0.001). Patients who received pharmacological treatment for delirium (n = 121, odds ratio (OR) 3.4, [2.1, 5.4], P < 0.001), who were affected by acute memory impairment (n = 149, OR 2.8, [1.8, 4.5], P < 0.001), or change in perception (n = 137, OR 2.9, [1.8, 4.6] P < 0.001) had higher odds for D-DD. In contrast, post-operative cases (OR 0.2, [0.1, 0.4], P < 0.001) had lower odds for D-DD. Conclusion: Underdiagnosis of in-hospital delirium was a major issue in our study, especially in less severe delirium cases. Our findings emphasise the need for integrating systematic delirium diagnostics and documentation into hospital admission and discharge routines. | en_US |
| dc.language.iso | eng | en_US |
| dc.publisher | Oxford University Press | en_US |
| dc.rights | Navngivelse 4.0 Internasjonal | * |
| dc.rights.uri | http://creativecommons.org/licenses/by/4.0/deed.no | * |
| dc.title | Delirium is frequently underdiagnosed among older hospitalised patients despite available information in hospital medical records | en_US |
| dc.type | Peer reviewed | en_US |
| dc.type | Journal article | en_US |
| dc.description.version | publishedVersion | en_US |
| dc.rights.holder | © The Author(s) 2024 | en_US |
| dc.source.volume | 53 | en_US |
| dc.source.journal | Age and Ageing | en_US |
| dc.source.issue | 2 | en_US |
| dc.identifier.doi | 10.1093/ageing/afae006 | |
| dc.identifier.cristin | 2245792 | |
| dc.source.articlenumber | afae006 | en_US |
| cristin.ispublished | true | |
| cristin.fulltext | original | |
| cristin.qualitycode | 2 |
Tilhørende fil(er)
Denne innførselen finnes i følgende samling(er)
-
Import fra CRIStin [3586]
-
Institutt for helse- og omsorgsvitskap [2723]

Med mindre annet er angitt, så er denne innførselen lisensiert som Navngivelse 4.0 Internasjonal